
MFN Update, Part 3: Strategic Implications
You’re a Market Access executive – what's your new ex-US strategy?
TLDR
MFN1 is likely to make biopharma companies more cautious about ex-US drug launches and access. As a quick refresher - under MFN, low drug prices abroad could reset US prices to lower levels.
In the short term, this will likely reduce global drug access to protect the US market.
In the long run, MFN will push manufacturers to better defend ex-US prices after launch and explore novel access channels (e.g., direct-to-consumer).
Setup: You’re a Market Access executive
Let’s pretend you’re a Market Access executive at Good Drug Co.
Your drug (“Healzalot”) has been very successful in the US, and now you need to decide on a global access strategy - including whether to launch in other countries.
You think to yourself:
Gosh, a few years ago this would have been a no-brainer. Sure drug prices are a lot lower in other countries, but we’d still make a profit on every prescription. Now with MFN, we really need to re-think our global strategy.
Your immediate reaction: “Will launching abroad hurt our US business?”
The first question on your mind is whether launching abroad (we’ll use France as our example) will put the US Healzalot market in harm’s way.
The new launch equation in your head starts to look like:
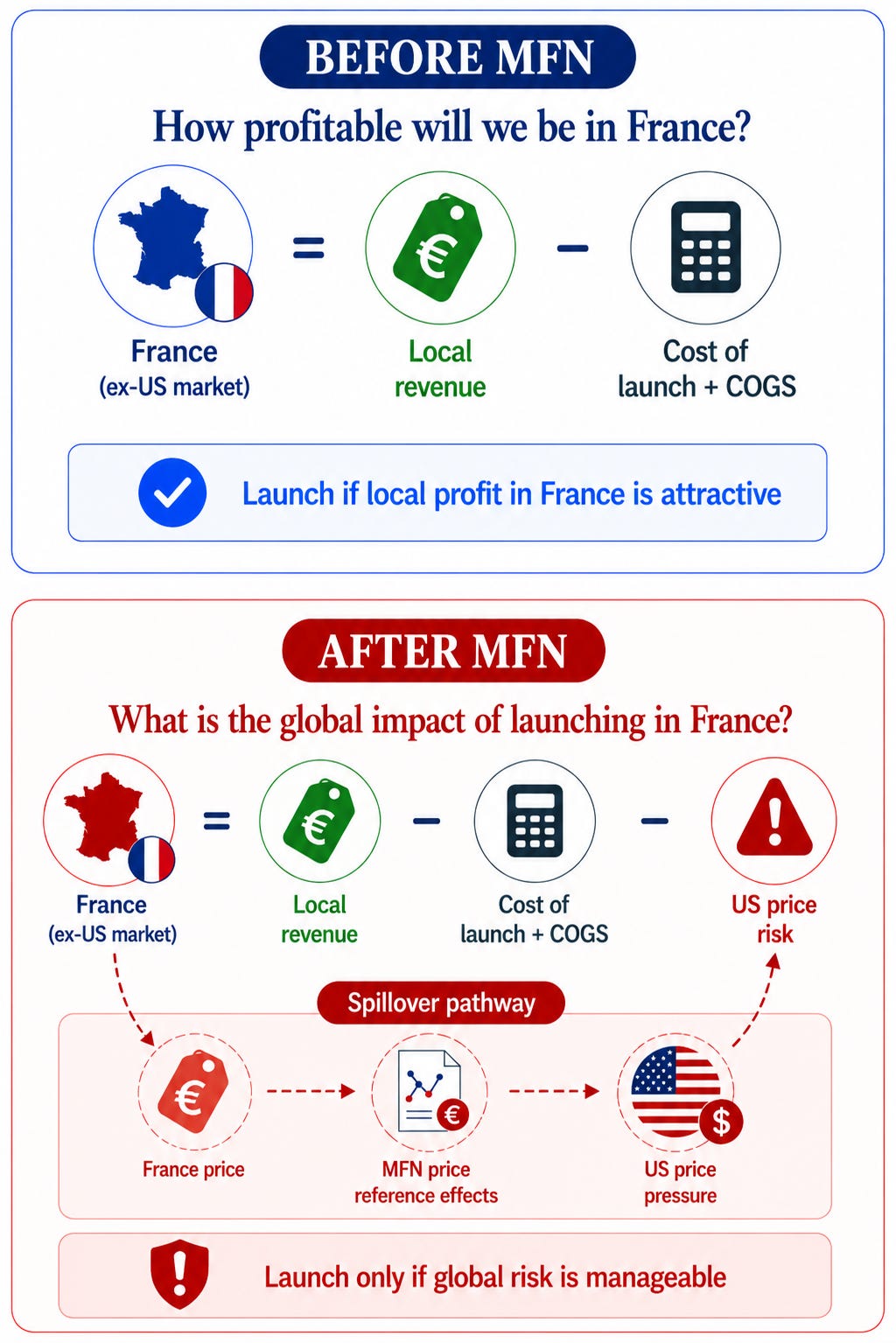
How would lower ex-US prices impact US revenues?
Today in the US, we get $200 for each Healzalot prescription. But if we launch in France, we might only get $100 there.2
If that pulls our US price down to $100, how much US revenue would we lose? How many patients would we have to treat in France to “break even”?
If $100 is too low, what’s our actual breakeven price? If France won’t meet that, should we just not launch in France at all? Or wait until our US price comes down?
Can we preserve access without creating a low reference price?
Maybe France won’t pay more than our breakeven price, but are there any other workarounds that would protect our US price under MFN?
Could we try to get a higher list price, but negotiate confidential rebates, volume caps, outcomes-based agreements, or programs to give away free product?
Could we market a different formulation (e.g., pill, auto-injector) in ex-US countries?
Could we secure an MFN carve-out for Healzalot in our upcoming negotiation with the Trump Administration?
If we do skip France, should we reduce our investments there?
It costs a lot of money to build manufacturing plants and run clinical trials. But if we’re selling fewer drugs in France, maybe we don’t need as many factories or clinical trials there.
Should we move those investments to countries with more favorable pricing and access environments?
Should we still sell ex-US commercial rights?
We were thinking about selling the ex-US commercial rights for Healzalot. JCA and HTA reviews are costly and time-intensive, and our forecasts don’t show a high return on investment in Europe.
But now I’m not so sure that’s a good idea.
What if we sell those rights and the buyer negotiates low ex-US prices? We wouldn’t have any input into those negotiations, which could be a big risk for us.
We’ll have to be very careful with how we structure those contracts in the future.
Looking ahead: “How can we better defend ex-US prices over time under MFN?”
Let’s say you move ahead with launching Healzalot in France. Your next questions are focused on how MFN will impact your post-launch strategies.
It’s one thing for the economics to line up at launch. But what if ex-US prices drop through the floor in three years when Healzalot is reassessed?
How can you prevent that from happening?
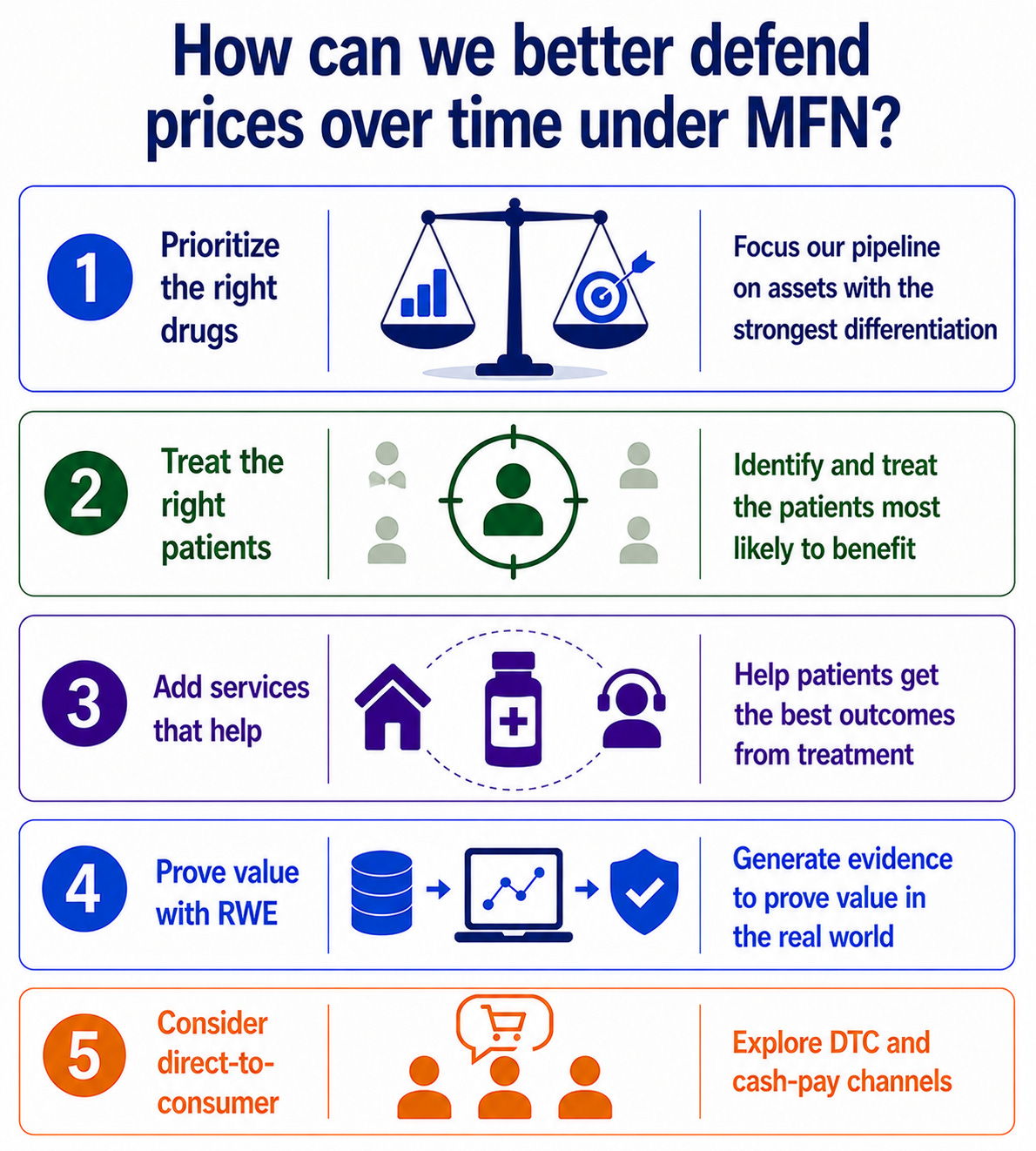
How will we prove the value of Healzalot in three years?
If Healzalot is reassessed in three years and prices are lowered, that could still hurt us in the US market.
Is there more real-world evidence we can generate to prove that Healzalot is improving outcomes in France?
Are there national data sources we can tap into, like the SNDS? Can we partner with an existing registry to show this? Do we need to set up our own registry?
Should we narrow access to the patients that will benefit most?
Should we make sure Healzalot treatment in France is focused on the patients most likely to benefit?
That could keep value per treated patient high and strengthen the evidence base when Healzalot is reassessed in a few years.
Could we use diagnostics, biomarkers, or AI tools to predict who will have the best response? How would this actually work in clinical practice?
What services can we offer with Healzalot that will improve outcomes?
Healzalot is a great drug on its own, but can we offer any companion services that will lead to even better outcomes?
Can we offer at-home infusions that will improve adherence?
Can we provide extra education or lifestyle coaching that will help patients get more mileage out of every treatment?
Should we consider direct-to-consumer channels outside the US?
This might have sounded far-fetched a few years ago, but this model has really taken off for some drugs in the US. If governments won’t pay the price we think Healzalot deserves, should we build a path for patients to pay themselves?
If we go down this path, we’ll need to make a compelling case directly to patients that Healzalot is good value for money and worth paying for out-of-pocket.
Do drugs like Healzalot still make sense for us?
We want to be paid fairly for developing innovative drugs, but countries also have fixed budgets and drugs are competing with schools, roads, defense, and many other spending priorities.
Other countries may never be willing to pay the price we think Healzalot deserves. So should we keep investing in drugs like Healzalot?
Or should we revisit our pipeline and shift investment toward drugs that are more differentiated and easier for governments to justify funding?
And if we start pulling back more broadly from ex-US markets, who’s going to fill the gap? I haven’t spent much time thinking about the Chinese biotech ecosystem, but should we be taking these companies more seriously as a competitive threat?
This article builds on three earlier pieces: 1) the MFN framework, 2) MFN’s warped curve effects, and 3) the early impacts of MFN. These are helpful primers if you’re just getting caught up on MFN!
For simplicity, we’ll also use “MFN” as shorthand for the full gamut of US reference-pricing policies that are emerging, including bilateral agreements, GENEROUS, and GLOBE / GUARD
To keep us from getting bogged down, I’m handwaving over a lot of nuance here. Like the fact that drugs in France will be paid for in Euros, not US dollars! :)
Or that reference prices will be adjusted for purchasing power parity (PPP), GENEROUS vs. GLOBE / GUARD having different reference countries and prices, retrospective vs. prospective MFN, etc.
Those are all (very) important details, but we’re going to gloss over them today to make our points more digestible. Thanks for bearing with me!